
Surgical Best Practice Spotlight: Vaginal Cuff Closure in Minimally Invasive Hysterectomy
![]()
![]() Theator
on
July 11, 2024
Theator
on
July 11, 2024
Extreme surgical variability exists in minimally invasive hysterectomies
About 600,000 hysterectomies are performed annually in the US, making it one of the most commonly performed surgical procedures, but the surgical practices performed within the procedure are anything but common.
For example, a previous Spotlight analysis surfaced that bilateral view of the ureter, a common surgical practice, is only achieved 54%f of the time. That got us thinking, what additional surgical practices should we be looking at in this procedure?
The answer? Vaginal cuff closure.
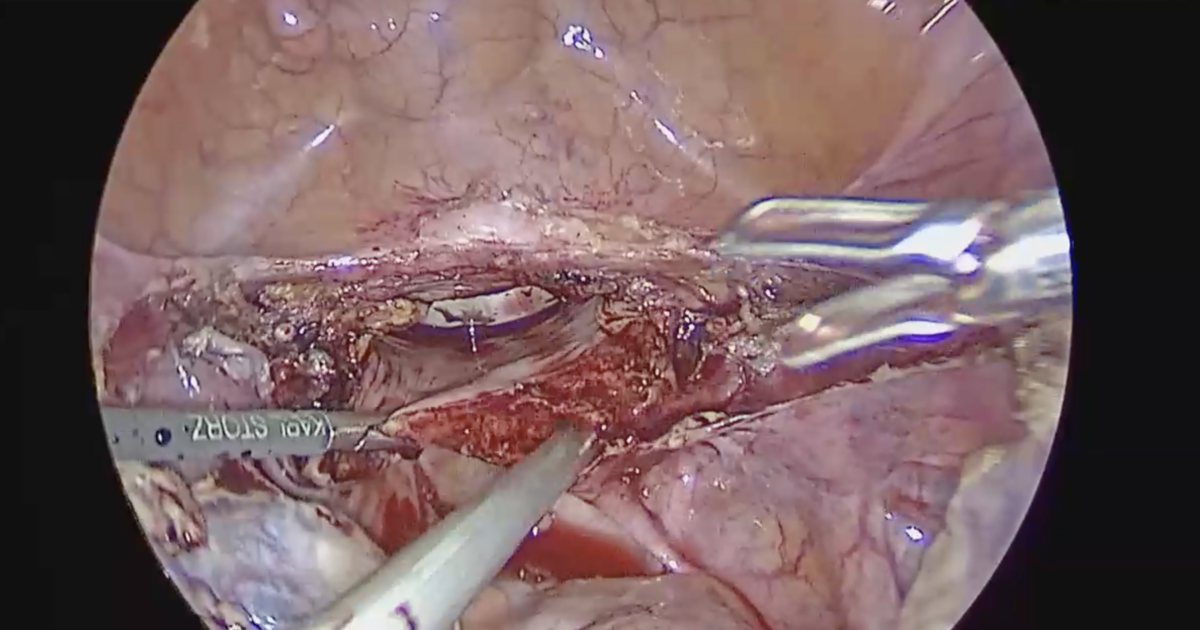
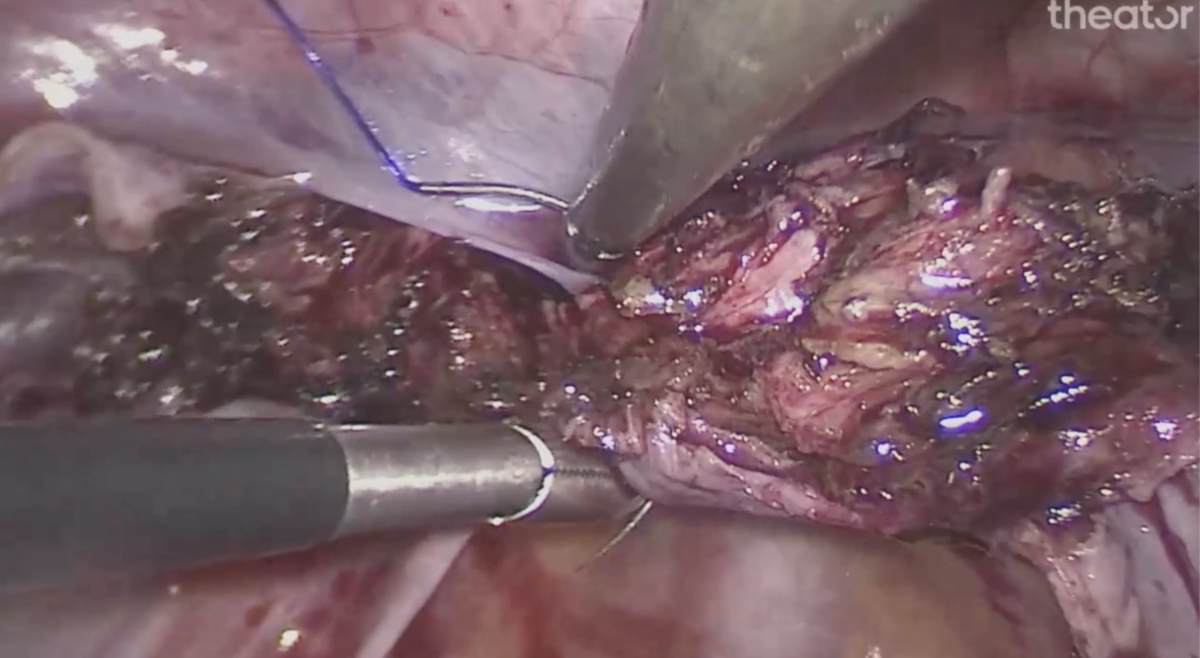
Vaginal Cuff Closure: A Surgical Best Practice
Vaginal cuff closure is a surgical best practice in hysterectomies, and multiple techniques and materials can be used to complete this step. Both a one-layer and two-layer technique are used in clinical practice, however, multiple studies indicate that the two-layer technique is associated with lower rates of complications, including:
- Infection
- Hematoma
- Need for blood transfusion
- Cuff complications (biggest contributing factor)
We analyzed 1,767 minimally invasive hysterectomies to find out which vaginal cuff closure techniques surgeons are using today. Download the report here. (It’s free!)
Vaginal cuff dehiscence after hysterectomy
Of the cuff complications noted above, vaginal cuff dehiscence is of particular concern. This refers to the partial or complete separation of previously sutured vaginal cuff edges, a rare but potentially fatal complication following hysterectomy. Importantly, vaginal cuff dehiscence occurs more often with one-layer than two-layer vaginal cuff closure.
Given that the two-layer technique results in decreased rates of vaginal cuff dehiscence, you may think this approach is favored in clinical practice and widely employed by gynecologists. However, our data shows, spoiler alert, that this occurs far less often than bilateral view of the ureter.
Theator’s Spotlight database compiled 1,767 hysterectomy procedures from 170 surgeons at 5 different health systems to investigate how often a two-layer vaginal cuff closure was achieved.
Curious how vaginal cuff closure techniques vary across health systems? How about within the same health system? Us too. We have answers – download the report here.
Surgical Intelligence and Gynecologic Surgery
![]()
![]() Theator
on
April 29, 2024
Theator
on
April 29, 2024
What Are The Advantages of AI in Gynecologic Surgery?
As the role of AI-enabled tools in surgical care expands, clinical research continues to validate the benefits of integrating streamlined AI technologies into operating rooms. In gynecology, surgical AI integration has the potential to improve quality of care and patient outcomes. A win-win.
What is Surgical Intelligence?
Surgical Intelligence is the analysis of surgical video data using AI that can surface insights that aren’t possible with manual data analysis alone. Its ability to identify specific and actionable measures to improve patient outcomes is why this technology is the future of surgical care.
Why Surgical Intelligence for gynecologic surgery?
Surgical Intelligence offers a number of advantages for clinicians and patients related to gynecologic surgeries.
Surgical step identification:
The ability of AI to identify the steps of a surgical procedure by analyzing video data is the first step toward harnessing this data to support clinicians and improve outcomes.
Specific to laparoscopic hysterectomy, available AI technologies demonstrated a 92% concordance between human and AI-directed annotation of surgical steps in one study, while a separate study found a similar 93% concordance rate between humans and AI-enabled technology in annotation of surgical steps.
The ability of AI to detect surgical steps significantly cuts down on the amount of time that would be required for humans to manually perform this task. This, in turn, allows for recorded surgical videos to be used more effectively to bolster the knowledge base and skill set of trainees.
Continuous quality improvement:
AI demonstrates a high rate of accuracy in identifying the surgical steps of a laparoscopic hysterectomy. This is notable because when AI is able to correctly identify these steps and landmarks in real time, it can then be trained to provide clinical decision support at the point of care.
For example, identification of the ureters is a critical step to avoid ureteral injury in laparoscopic hysterectomy. However, this step isn’t universally performed during this procedure. By surfacing this information to a hospital’s gynecology department, a proactive, data-driven quality initiative can be implemented to drive adoption of this surgical practice—therefore increasing the safety of laparoscopic hysterectomy procedures.
Outcomes assessment:
Because Surgical Intelligence integrates with patient outcomes data, it offers the opportunity to link what happens in the OR to outcomes such as infections, readmissions, reoperations, and increased length of stay. This allows healthcare organizations to identify systemic and individual areas for quality improvement.
Surgical Intelligence represents the future of care in all surgical specialties. By effectively and efficiently identifying procedural steps, AI-enabled tools have the power to assist clinicians with making evidence-based decisions at the point of care. Furthermore, they can link this data to patient outcomes to identify how intraoperative events affect what happens after surgery. The potential benefits of this technology for gynecologic (and all other) surgeries are significant, and staying ahead of the curve with Surgical Intelligence will benefit surgeons and patients alike.
Surgical Spotlight: Laparoscopic Hysterectomy
![]()
![]() Theator
on
April 17, 2024
Theator
on
April 17, 2024
Laparoscopic Hysterectomy Insights
Laparoscopic hysterectomy is performed for a variety of indications, the most common of which is symptomatic uterine fibroids. In just over two decades, hysterectomies in the US went from being performed via an open abdominal approach in 70% of cases to being performed laparoscopically 70% of the time.
The laparoscopic approach to hysterectomy offers a number of advantages over open abdominal hysterectomy, including reductions in:
- Recovery time
- Pain
- Blood loss
- Costs
However, like all surgical procedures, laparoscopic hysterectomy has a risk of complications including:
- Urinary tract injury
- Bowel injury
- Vascular injury
- Bleeding
Readmission within 30 days following laparoscopic hysterectomy occurs in 2.6% of patients, with most of these occurring within the first 15 postoperative days. Surgical site infection (28.3%) is the most common reason for readmission. Notably, 51.9% of complications following laparoscopic hysterectomy are related to infections, surgical injuries, and wound complications, which are all potentially preventable outcomes.
These complications can affect patients both physically and emotionally, as well as increase the cost of care.
For more laparoscopic hysterectomy insights, download our procedure spotlight report.
Surgical Practices in Laparoscopic Hysterectomy
Identification of critical anatomic landmarks is an essential step in preventing surgical complications associated with laparoscopic hysterectomy. For example, identification of the bilateral ureters can prevent injury to these structures.
However, this step isn’t universally performed by all surgeons, and rates of bilateral ureter identification vary by institution. Theator’s Surgical Intelligence database has compiled more than 1150 laparoscopic hysterectomies to date from 9 different health systems, and we’ve found rates as low as 37% and as high as 72% for identification of both ureters at different institutions.
This is just one metric that Theator’s Surgical Intelligence Platform recognizes, analyzes, and connects to health system outcomes so hospital administrators and surgeons can take a data-driven approach to improving the quality of surgical care.
Curious to know what other insights we’ve seen in our database of laparoscopic hysterectomies? Download the full report here

