Surgical Spotlight: Gastric Bypass
![]()
![]() Jordan
on
October 4, 2024
Jordan
on
October 4, 2024

Bariatric surgery is growing, but gastric bypass procedures remain stable
Bariatric surgery is growing in volume year-over-year, but the volume of Roux-en-Y gastric bypasses, or ‘gastric bypass’ for short, has remained relatively stable over the past few years. In total, gastric bypass procedures account for approximately 20% of all bariatric procedures. Sleeve gastrectomies make up the majority of that difference and are the most common. Even though sleeve gastrectomies are simpler to perform and more straightforward surgery, significant variability still exists.
A gastric bypass procedure, on the other hand, modifies a patient’s digestive system to consume and absorb fewer calories. It is more complex and surgically challenging than sleeve gastrectomies, but interestingly, many of the surgical practices for Roux-en-Y gastric bypasses have high adoption.
Variability in procedure duration
As we found with sleeve gastrectomy procedures, procedure duration widely varies, and that variability is exacerbated when performed robotically vs. laparoscopically. In reviewing over 300 gastric bypass procedures across 4 health systems, the median procedure time varied from 68 minutes as the shortest, to 133 minutes as the longest. How is surgical practice adoption impacted by procedure time? Fast-forward to our findings by downloading here.
Performing the safest gastric bypass procedure
There are seven surgical practices defined in peer-reviewed literature to increase the surgical quality of a gastric bypass procedure that Theator’s Surgical Intelligence Platform automatically annotates. In this Theator Spotlight edition, two of them are thoroughly analyzed:
- Closing the mesenteric defect
- Intraoperative leak test
Closing the mesenteric defect
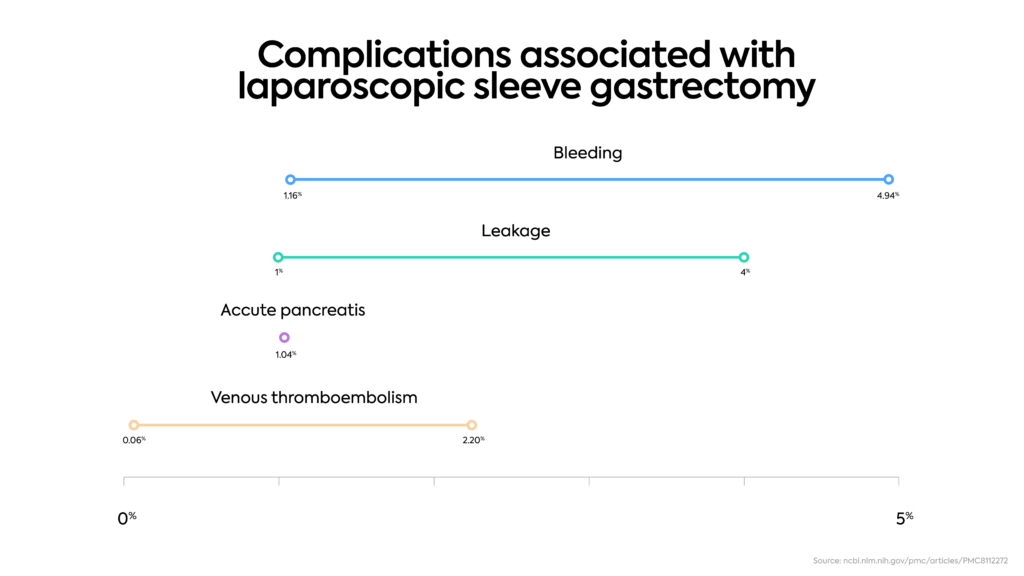
A common complication that carries significant morbidity after a gastric bypass procedure is a small bowel obstruction. In one study, closure of the mesenteric defects can reduce the incidence of small bowel obstruction by approximately 48%. While overall adoption is high, significant variability exists between health systems, with one achieving this surgical best practice less than 70% of the time.
Intraoperative leak test
Reducing the risk of anastomotic leaks is at the top of surgeons’ minds. A surgical practice to mitigate this risk is performing an intraoperative leak test on the gastrojejunal anastomosis. Three out of the four health systems analyzed performed this practice the majority of the time, yet variability exists in how this practice is performed.
Despite an overall high adoption of these two surgical practices in gastric bypass, significant variability exists across health systems. Check out the full report here.